Page 1 of 107
THE CITY OF NEW YORK
DEPARTMENT OF FINANCE
OFFICE OF THE SHERIFF
30-10 Starr Avenue, 2
nd
Floor
Long Island City, NY 11101
(718) 707-2000
BACKGROUND INVESTIGATION QUESTIONNAIRE
DEPARTMENT OF FINANCE, OFFICE OF CITY SHERIFF BACKGROUND INVESTIGATIONS ARE DETAILED AND THOROUGH.
INFORMATION PROVIDED BY INDIVIDUALS IN THE BACKGROUND QUESTIONNAIRE IS VERIFIED BY THIS DEPARTMENT WITH
OUTSIDE AGENCIES. FOR EXAMPLE, CRIMINAL CONVICTIONS ARE VERIFIED WITH THE FEDERAL BUREAU OF INVESTIGATION
AND/OR THE NEW YORK STATE DIVISION OF CRIMINAL JUSTICE SERVICES; TAX FILING DATES ARE VERIFIED WITH THE INTERNAL
REVENUE SERVICE AND THE NEW YORK STATE DEPARTMENT OF TAXATION AND FINANCE; EDUCATIONAL DEGREES ARE
VERIFIED WITH SCHOOLS AND UNIVERSITIES; AND EMPLOYMENT HISTORY IS VERIFIED WITH PREVIOUS EMPLOYERS, ETC.
A FALSE STATEMENT OR INTENTIONAL OMISSION MADE IN THIS QUESTIONNAIRE OR IN CONNECTION WITH THIS
BACKGROUND INVESTIGATION MAY RESULT IN THE IMPOSITION OF DISCIPLINARY PENALTIES, INCLUDING TERMINATION OF
EMPLOYMENT, OR DISQUALIFICATION FROM FUTURE EMPLOYMENT AND, IN ADDITION, MAY SUBJECT YOU TO CRIMINAL
PROSECUTION.
THIS DEPARTMENT WILL NOT APPROVE YOUR TERMS AND CONDITIONS OF APPOINTMENT IF YOU FAIL TO PROVIDE ALL
INFORMATION REQUESTED OR OTHERWISE FAIL TO COOPERATE FULLY IN THIS INVESTIGATION.
PLEASE KEEP A COPY OF THIS FORM FOR YOUR RECORDS FOR AT 10 YEARS.
THIS BACKGROUND INVESTIGATION QUESTIONNAIR (BIQ) IS NOT A PUBLIC DOCUMENT AND CANNOT BE ACCESSED BY THE
PUBLIC THROUGH THE FREEDOM OF INFORMATION LAW (FOIL).
For Sheriff Use Only
Candidate:
Candidate Telephone #:
Investigator:
Background Interview Date: / /
Sheriff Review Date: / /
Page 2 of 107
TABLE OF CONTENTS
INSTRUCTIONS 003
ELIGIBITY REQUIREMENTS 004
REQUIRED DOCUMENT CHECKLIST 006
PERSONAL INFORMATION 009
FAMILY AND HOUSEHOLD INFORMATION 015
MAITAL STATUS AND RELATIONSHIPS 021
RESIDENCE 027
DRIVING HISTORY 031
ACADEMIC/EDUCATIONAL RECORD 041
EMPLOYMENT HISTORY 043
MILITARY SERVICE 055
CIVIL AND CRIMINAL INVESTIGATIONS HISTORY 059
TAX INFORMATION AND FINANCIAL STATUS 071
APLICATIONS TO GOVERNMENT AGENCIES 081
FIREARMS LICENSES AND PERMITS 087
MISCELLANEOUS 091
CERTIFICATION AND SIGNATURE 100
FIREARMS SECURITY FORM 101
DOMESTICE VIOLENCE INQUIRY FORM 103
NOTICE TO CANDIDATES 105
AUTHORIZATION FOR RELEASE OF INFORMATION FORM 107
Page 3 of 107
BACKGROUND INVESTIGATION QUESTIONNAIRE INSTRUCTIONS
Dear Candidate,
The Background Investigation phase of The City of New York, Department of Finance, Office of the Sheriff recruitment
effort is about to begin. In order to help facilitate this process, you are being supplied with the Required Document
Checklist in advance of your Background Investigation Interview.
This checklist will not only let you know what you are required to provide but will also provide guidance on where to begin
your search for these items. Please use the checklist to collect all the information listed, as some of the information
required may not be readily accessible to you and may take some time to obtain. Take time to organize your paperwork
(original and photocopies) in the order listed on the checklist.
Additionally, you are required to provide answers to the questions contained in this Background Investigation
Questionnaire. All answers must be clearly handwritten in blue ink or TYPED.
This Background Investigation Questionnaire is to be completed in its entirety. If additional space is required to
complete your answer to any question, additional space is provided at the end of this application. There, indicate the
question number and continue your answer. If any question does not apply to you, mark the answer section with N/A or
None. NO QUESTION IS TO BE LEFT UNANSWERED AND NO ANSWER SECTION IS TO BE LEFT BLANK.
Candidates are required to answer each question truthfully, completely and without evasion. Failure to do so may result in
your disqualification from the hiring process.
For the purpose of this application and background investigation, the word "discipline" shall include ANY action taken by
an employer, volunteer organization, school, agency, department, branch, institution, organization, or ANY OTHER
ENTITY of which the candidate is associated with or a member. The word "arrest" includes any "detaining, holding, or
taking into custody by any police or law enforcement agency" of a person in order to answer for the alleged
performance or commission of any "charge, offense and/or crime" in ANY jurisdiction, whether foreign or domestic.
Offenses include felonies, misdemeanors, violations and all criminal court summons. A guilty plea, guilty verdict,
or plea of nolo contendere is a conviction even if, upon sentencing, you were never imprisoned, only paid a fine, were
conditionally or unconditionally discharged, or received a Certificate of Relief from Disabilities. You MUST disclose any
material sealed, expunged, or set aside under Federal or State law, or any juvenile delinquent or youthful
offender adjudications.
When you arrive at your Background Investigation Interview, you will be required to provide the completed Background
Investigation Questionnaire, one (1) photocopy and the original of each item on the document checkoff list. Photocopy
only ONE (1) ITEM PER PAGE. Each photocopy must be neat, clear, and legible and on “8½ X 11” paper. Any
photocopies larger than this or that are not neat, clear, and legible WILL NOT BE ACCEPTED. The original will be
examined against the photocopy that you are to provide and then immediately returned to you. You WILL NOT have the
opportunity to make photocopies on this day. PROVIDE ONE (1) COLOR PASSPORT PHOTO. DO NOT STAPLE
ANY PAGES.
If you have any questions related to what you will need for the Background Investigation Questionnaire, review your copy
of the required Document Checklist to see if it is answered there. If you still have questions about what you need for
Background Investigation Questionnaire after reviewing the checklist, you may then contact Deputy Cadet Processing at
DeputySheriffCand[email protected].gov. ALL OTHER QUESTIONS WILL BE ANSWERED AT THE BACKGROUND
INVESTIGATION INTERVIEW.

Page 4 of 107
ELIGIBILITY REQUIREMENTS
Education and Experience Requirements: By the time you are appointed to this position, you must have:
1. a baccalaureate degree from an accredited college or university; or
2. a four-year high school diploma or its educational equivalent and two years of honorable full-time U.S.
military service or two years of satisfactory, full-time professional or paraprofessional experience in law
enforcement, civil enforcement, criminal justice, law, accounting, auditing, investigation, public
administration, business administration, or a closely related field; or
3. a satisfactory combination of education and/or experience that is equivalent to “1" or “2" above. College education can
be substituted for the required experience in “2" above on the basis that each 30 semester credits is equated to six
months of experience. However, all candidates must have a four-year high school diploma or its educational equivalent.
The high school diploma or its educational equivalent must be approved by a State's Department of Education or a
recognized accrediting organization. The college or university must be accredited by regional, national, professional, or
specialized agencies recognized as accrediting bodies by the U.S. Secretary of Education and by the Council for Higher
Education Accreditation (CHEA).
If you were educated outside the United States, you must have your foreign education evaluated to determine its
equivalence to education obtained in the United States. You will receive instructions from the Department of Finance
during the pre-employment screening process regarding the approved evaluation services that you may use for foreign
education.
Peace Officer Status and Training: You must satisfy the requirements established by the State of New York for Peace
Officers. You must meet and maintain the requirements for Peace Officer status for the duration of your employment. You
must successfully complete a course of peace officer training which includes instruction in deadly physical force and the
use of firearms and other weapons and will be required to carry a firearm on duty.
Firearms Qualifications: You must qualify and remain qualified for firearms usage and possession as a
condition of employment for the duration of your employment. Failure to qualify and remain qualified for
firearms usage and possession may result in termination.
Driver License Requirement: By the time you are appointed to this position, you must have a motor vehicle driver
license valid in the State of New York with no restrictions that would preclude the performance of Deputy City Sheriff work.
If you have moving violations, license suspension(s) or an accident record, you may be disqualified. This license must be
maintained for the duration of your employment.
Medical and Psychological Requirement: Medical and psychological guidelines have been established for the position
of Deputy City Sheriff. Candidates will be examined to determine whether they can perform the essential functions of the
position of Deputy City Sheriff. Where appropriate, a reasonable accommodation will be provided for a person with a
disability to enable him or her to take the examination, and/or to perform the essential functions of the job.
Physical Fitness Requirement: You will be required to pass a qualifying physical test.
Drug Screening Requirement: You must pass a drug screening in order to be appointed.
Residency Requirement Advisory: The New York State Public Officers Law requires that any person employed as a
Deputy City Sheriff in New York City must be a resident of the City of New York or of Nassau, Westchester, Suffolk,
Orange, Rockland, or Putnam counties.

Page 5 of 107
ELIGIBILITY REQUIREMENTS (continued)
English Requirement: You must be able to understand and be understood in English.
Proof of Identity: Under the Immigration Reform and Control Act of 1986, you must be able to prove your
identity and your right to obtain employment in the United States prior to employment with the City of New
York.
Citizenship Requirement: United States citizenship is required at the time of appointment to Deputy City
Sheriff.
Character and Background: Pursuant to Criminal Procedure Law Section 2.10, the position of Deputy City Sheriff is
designated as a Peace Officer position. Accordingly, proof of good character is an absolute prerequisite to appointment
since eligible candidates must meet the requirements for Peace Officer status after successful completion of a prescribed
training course. Therefore, you must reveal ALL arrests, convictions and pending charges that have occurred in your
lifetime. This includes any material sealed, expunged, or set aside under Federal or State law, or juvenile delinquent or
youthful offender adjudications. The following are among the factors which may be cause for disqualification: (a)
conviction of an offense, the nature of which indicates lack of good moral character or disposition toward violence or
disorder, or which is punishable by one or more years of imprisonment; (b) two or more convictions of an offense, where
such convictions indicate disrespect for the law; (c) discharge from employment, where such discharge indicates poor
behavior or inability to adjust to discipline; (d) dishonorable discharge from the Armed Forces.
Age Requirements: You must have reached your 18th birthday by the time of appointment.
Investigation: This position is subject to investigation before appointment. At the time of investigation, you will be
required to pay a $75.00 fee for fingerprint screening. At the time of investigation and at the time of appointment, you must
present originals of certified copies of all required documents and proof, including, but not limited to, proof of date and
place of birth by transcript of record of the Bureau of Vital Statistics or other satisfactory evidence, naturalization papers, if
necessary, proof of any military service, and proof of meeting educational requirements. Any willful misstatement or failure
to present any documents required for investigation will be cause for disqualification.
Page 6 of 107
REQUIRED DOCUMENT CHECKLIST
☐ Background Investigation Questionnaire
☐ NYS Driver License
☐ Registrations for all vehicles currently owned/leased/operated by you
☐ Insurance paperwork for all vehicles currently owned/leased/operated by you
☐ DMV Lifetime Abstract
☐ Birth Certificate
☐ Naturalization Certificate
☐ All Records of Change in Name (if applicable)
☐ Proof of Residence (e.g., Rental/Mortgage Paperwork, Bank Statement, Service Bills)
☐ Marriage License or Divorce Decree/Separation Paperwork
☐ Social Security Card
☐ Social Security Earnings Information (certified detailed itemized earnings statement)
☐ Certificate of Release or Discharge from Active Duty (DD214) for each period and each component of service that
shows the following:
A) Type of separation
B) Character of service
C) Separation code
D) Reentry code
☐ SF-180 Request Pertaining To Military Records
☐ Selective Service Verification
☐ High School Diploma or GED Certificate
☐ College Diploma(s)
☐ Official Sealed College Transcripts
☐ Any and All Arrest(s) Paperwork, including but not limited to:
A) arrest report/summonses

Page 7 of 107
B) court dispositions
C) proof of satisfaction
D) notarized statement
☐ Most Updated Resumé
☐ Unemployment Documentation for Compensation for Any Periods of Unemployment
☐ Federal and State Tax Returns Transcripts for past 10 Years
☐ Copy of personal credit report (less than 30 days old) from ONE (1) of the three major credit reporting agencies
A) Equifax
B) Experian
C) TransUnion
☐ Professional License/Certificates
☐ Weapons Permits (e.g., firearms ID, purchase permit, conceal carry permit) along with proof of ownership for any and
all weapons including disposition for all weapons owned, sold and/or traded)
☐ Vehicular Accident Reports, along with notarized statements explaining them
☐ Documentation regarding status with any and all government agency applications/tests taken
☐ Inquiry Regarding Conviction for Misdemeanor Crimes of Domestic Violence
☐ Notarized Firearms Security Form
☐ Notarized Authorization for Release of Information
NOTE: If any paperwork cannot be provided to us within the time frame given, please show receipt for that
particular paperwork as proof that obtainment is pending
The burden of obtaining and providing said documents is the responsibility of the applicant’s and
NOT the NYC Department of Finance or NYC Sheriff’s Office

Page 8 of 107
THIS PAGE
IS INTENTIONALLY LEFT
BLANK
Page 9 of 107
INSTRUCTIONS
All questions must be answered completely and accurately. Type or
print clearly in blue ink. If you need more space, on the back of every
question sheet is an addendum for additional space for you to use.
Indicate if a question is inapplicable to you by entering N/A.
This BIQ must be signed and sworn to by you before a Notary Public or
Commissioner of Deeds.
Attached here passport-size
photograph taken within the
past twelve (12) months.
PERSONAL INFORMATION
1A. Full Name
1B. Have you ever used or been known by any other name, including a maiden name?
Yes☐ No☐
If yes, provide the information requested below:
2. Date of Birth:
_______/_______/_______
Month Day Year
3. Place of Birth:
4A. Social Security Number:
4B. Have you ever used, or been issued, a Social Security number other than the one listed
above? Yes☐ No☐
If yes, list the other Social Security number(s) used or issued, and provide details including
dates and reasons used or issued below:
Page 10 of 107
Additional Space
Page 11 of 107
Hair Color
Eye Color
Height (Feet/Inches)
Weight (pounds)
List ALL Scars, Marks and Tattoos/Body Art (Provide location on body, description and meaning for all)
Street Address
City, State, Zip Code
Residence Phone Number
Cellular Phone Number
Work Phone Number
Personal Email
Work Email
7. Contact Information:
5. Physical Features:
6. Current Physical Address:
Page 12 of 107
Additional Space
Page 13 of 107
Certificate #
Alien Registration #
Date of
Issuance
Month / Day
/ Year
Court of Issuance
8A. Are you currently a U.S. Citizen?
Yes☐ No☐
If you are not a U. S. citizen, then state the country of your citizenship:
Country of Citizenship: ____________________________________________________
8B. Are you legally present in the United States?
If you answered no, provide an explanation:
Yes☐ No☐
IF YOU ARE NOT A UNITED STATES CITIZEN, THEN BRING YOUR
ORIGINAL IMMIGRATION DOCUMENT(S) AUTHORIZING YOUR
ENTRY INTO, AND EMPLOYMENT IN, THE UNITED STATES WITH
YOU TO YOUR BACKGROUND INTERVIEW.
9. Are you a naturalized citizen? Yes☐ No☐
If yes you are a naturalized U.S. citizen, provide the following information:
IF YOU ARE A NATURALIZED CITIZEN OF THE UNITED STATES,
BRING YOUR ORIGINAL CERTIFICATE OF NATURALIZATION
WITH YOU TO YOUR BACKGROUND INTERVIEW.
Page 14 of 107
Additional Space
Page 15 of 107
11. Please provide the information regarding the following family member: Father
Full Name (Last Name, First Name, MI)
Physical Address
Date of Birth
Place of Birth
Occupation
Employer
Residence Phone Number Cellular Phone Number Work Phone Number
Full Name (Last Name, First Name, MI)
Physical Address
Date of Birth
Place of Birth
Occupation
Employer
Residence Phone Number Cellular Phone Number Work Phone Number
FAMILY AND HOUSEHOLD INFORMATION
10. Please provide the information regarding the following family member: Mother
Page 16 of 107
Additional Space
Page 17 of 107
Caretaker 1. Full Name (Last Name, First Name, MI)
Physical Address
Relation To You
Contact Phone Number
Caretaker 2. Full Name (Last Name, First Name, MI)
Physical Address
Relation To You
Contact Phone Number
Explanation for having been raised by person(s) other than biological parents
12A. Were you raised by family members, foster family or any others that are not your biological
parents? Yes☐ No☐
12B. If yes, provide the following for the caretaker.
Page 18 of 107
Additional Space
Page 19 of 107
Sibling 1: Full Name (Last Name, First Name, MI)
Physical Address
Date of Birth
Relation to You
Contact Phone Number
Sibling 2: Full Name (Last Name, First Name, MI)
Physical Address
Date of Birth
Relation to You
Contact Phone Number
Sibling 3: Full Name (Last Name, First Name, MI)
Physical Address
Date of Birth
Relation to You
Contact Phone Number
Person 1: Full Name (Last Name, First Name, MI)
Date of Birth
Relation to You
Contact Phone Number
Person 2: Full Name (Last Name, First Name, MI)
Date of Birth
Relation to You
Contact Phone Number
13. Please provide the information regarding the following family member(s): Sibling(s)
Any additional siblings may be added on the back of this page
14. Please provide the following information regarding any members living with you in your
household who are not part of your immediate family.
Page 20 of 107
Additional Space
Page 21 of 107
The individual listed below is my: Spouse ☐ Significant Other ☐ Domestic Partner ☐
Full Name (Last Name, First Name, MI)
Date of Birth
Date of Marriage
Location of Marriage (City, State or Country)
Current Physical Address
Residence Phone Number
Cellular Phone Number
Work Phone Number
The individual listed below was my: Spouse ☐ Significant Other ☐ Domestic Partner ☐
Full Name (Last Name, First Name, MI)
Date of Birth
Place of Birth
Date of Marriage
Location of Marriage
(City, State or Country)
Date of Divorce
Court/Agency Divorce
Filed With
Grounds for Divorce
Approximate dates for
relationship if unmarried
MARITAL STATUS AND RELATIONSHIPS
15A. Are you currently married, in a relationship with a significant other, or in a relationship with a
domestic partner? Yes☐ No☐
15B. If yes, please provide the following information.
16A. Other than your current marriage/relationship, were you ever married prior or been in a
relationship with a significant other and/or domestic partner? Yes☐ No☐
16B. If yes, provide the following information for the individuals from the previous relationship(s).
15C. Are you currently estranged or legally separated from the above?
No ☐ Yes, Estranged ☐ Yes, Legally Separated ☐ N/A ☐
Page 22 of 107
Additional Space
Page 23 of 107
The individual listed below was my: Spouse ☐ Significant Other ☐ Domestic Partner ☐
Full Name (Last Name, First Name, MI)
Date of Birth
Date of Marriage
Location of Marriage
(City, State or Country)
Date of Divorce
Court/Agency Divorce
Filed With
Grounds for Divorce
Approximate dates for
relationship if unmarried
The individual listed below was my: Spouse ☐ Significant Other ☐ Domestic Partner ☐
Full Name (Last Name, First Name, MI)
Date of Birth
Date of Marriage
Location of Marriage
(City, State or Country)
Date of Divorce
Court/Agency Divorce
Filed With
Grounds for Divorce
Approximate dates for
relationship if unmarried
Child’s Full Name (Last Name, First Name, MI)
Date of Birth
Relation
Child’s Current Residence
Parents’ Full Names (Last Name, First Name, MI)
17A. Do you have any children? Yes☐ No☐
17B. If yes, indicate number of children and/or stepchildren and provide the following information below.
Number of Children
Page 24 of 107
Additional Space
Page 25 of 107
Additional Children may be included on the back on this page.
Child’s Full Name (Last Name, First Name, MI)
Date of Birth
Relation
Child’s Physical Address
Parents’ Full Names (Last Name, First Name, MI)
Child’s Full Name (Last Name, First Name, MI)
Date of Birth
Relation
Child’s Physical Address
Parents’ Full Names (Last Name, First Name, MI)
Child’s Full Name (Last Name, First Name, MI)
Date of Birth
Relation
Child’s Physical Address
Parents’ Full Names (Last Name, First Name, MI)
Child’s Full Name (Last Name, First Name, MI)
Date of Birth
Relation
Child’s Physical Address
Parents’ Full Names (Last Name, First Name, MI)
Page 26 of 107
Additional Space
Page 27 of 107
Residence Address
Dates of Occupancy
From: To:
Residence Address
Dates of Occupancy
From: To:
Residence Address
Dates of Occupancy
From: To:
Residence Address
Dates of Occupancy
From: To:
Residence Address
Dates of Occupancy
From: To:
Residence Address
Dates of Occupancy
From: To::
Residence Address
Dates of Occupancy
From: To:
Residence Address
Dates of Occupancy
From: To:
RESIDENCE
18. List ALL addresses you have used in your lifetime, starting with your primary
residence, and work backwards chronologically. Indicate if you have a current mailing
address that is different from primary address. If applicable, state the addresses used
while serving the military and/or attending college during that specific time period.
Page 28 of 107
Additional Space
Page 29 of 107
Full Name
Relationship
Date of Birth
19. List ALL members of your current household, including immediate family and non-immediate family.
20A. Do you own or rent your primary address property? Own☐ Rent☐ Neither ☐
20B. If applicable, indicate monthly rent or mortgage:
If no monthly payment is made for primary residence property, explain why and/or how.
21. Have you ever lived in public housing (NYCHA) or received federal housing subsidies?
Yes☐ No☐
Page 30 of 107
Additional Space
Page 31 of 107
Name on License
License # / State
Address Recorded with DMV
DRIVING HISTORY
23. Do you have a driver’s license? Yes☐ No☐
If yes, list below all domestic and foreign driver’s licenses:
22. If you became an employee of the City of New York on or after January 4, 1973, and if, while so
employed, you were a nonresident of the City during any period of your employment, you are
subject to 1127 of the New York City Charter. This condition of employment mandates the filing
of Form NYC-1127 and payment of an amount equal to the City personal income tax computed as
if you were a resident of the City.
Have you filed Form NYC-1127 with the New York City Department of Finance for each year you were
subject to 1127 of the Charter and made payment of any amount due? Yes☐ No☐
If this question does not apply to you, then check the following box: N/A ☐
If no, provide details, including year(s) not filed and amount of any payment(s) due:
Page 32 of 107
Additional Space
Page 33 of 107
Year/Make
License Plate #
Name of Owner
Registration Address
Year/Make
License Plate #
Name of Owner
Registration Address
Yes☐ No☐
Note: Pursuant to New York State law, you may only possess one (1) U.S. driver’s license at
a time and if you have resided continuously in New York State for more than 30 days, you
must obtain a New York State driver’s license, as well as a New York State registration for
any vehicle(s) maintained within the State.
24. Have you had a driver’s license revoked or suspended?
25A. Do you or your spouse/significant other/domestic partner currently have (a) motor vehicle(s)
registered or leased in either of your names, or in the name of a business in which you or your
partner have an ownership interest? Yes☐ No☐
If yes, provide the following information
25B. Are there any other vehicles, such as cars owned by an employer, friend, or relative that you
regularly drive? Yes☐ No☐
If yes, provide the following information
Page 34 of 107
Additional Space
Page 35 of 107
Date of
Violation
License
State
Violation
Occurrence
State
Violations
Ticket Number
Reason of Violation
Date Issued
Amount Due
Reason Pending
$
$
$
$
Date Issued
Jurisdiction
Amount Due
Reason Pending
$
$
$
$
25A. List ALL traffic violations including but not limited to, any pending violations that did not result
in revocation/suspension, speeding violations, traffic device .
25B. List ALL outstanding parking violations with New York City Parking Violations Bureau (PVB).
Note: Candidates undergoing a background investigation MUST satisfy all outstanding parking
violations with PVB, either by making payment or be entering into a payment agreement. Attach
to this BIQ your proof of payment (receipt or canceled check) or a copy of your payment
agreement.
25C. List ALL outstanding parking and/or traffic violations in any jurisdiction outside New York City.
Page 36 of 107
Additional Space
Page 37 of 107
Date of Accident
Location of Accident
Responding
Agency/Agencies
Injuries
Result from Accident as Motor Vehicle Operator (e.g., cited at fault, summons issued, arrested)
If applicable, indicate what type of summons was issued and describe the accident.
Date of Accident
Location of Accident
Responding
Agency/Agencies
Injuries
Result from Accident as Motor Vehicle Operator (e.g., cited at fault, summons issued, arrested)
If applicable, indicate what type of summons was issued and describe the accident.
26. Were you ever involved in a motor vehicle accident where you acted as the operator?
Yes☐ No☐
If yes, list ALL motor vehicle accidents you were involved.
Page 38 of 107
Additional Space

Page 39 of 107
Date of Accident
Location of Accident
Responding
Agency/Agencies
Injuries
Result from Accident as Motor Vehicle Operator (e.g., cited at fault, summons issued, arrested)
If applicable, indicate what type of summons was issued and describe the accident.
Date of Accident
Location of Accident
Responding
Agency/Agencies
Injuries
Result from Accident as Motor Vehicle Operator (e.g., cited at fault, summons issued, arrested)
If applicable, indicate what type of summons was issued and describe the accident.
If there are additional motor vehicle accidents to add, you can include them on the back of this page
Page 40 of 107
Additional Space
Page 41 of 107
Institution Name
Location
(City, State or
Country)
Years Attended
(Month/Year)
Degree
Awarded
(Yes/No)
Type of
Degree
Date
Awarded
(Month /
Year)
From:
To:
From:
To:
From:
To:
From:
To:
From:
To:
From:
To:
From:
To:
From:
To:
From:
To:
ACADEMIC/EDUCATIONAL RECORD
27. List below all colleges, universities, graduate schools, professional schools, or technical
schools you attended. List them chronologically backwards until High School. If you have
received a degree from a foreign educational institution, attach to this BIQ a copy of the
original degree and a certified translation. If you have not received a college degree, list high
school(s) attended and indicate if a diploma or equivalency diploma was awarded.
Page 42 of 107
Additional Space
Page 43 of 107
Institution Name
Date of
Discipline or
Investigation
Reason for Discipline or
Investigation
Result of Discipline or
Investigation
28. Were you ever disciplined or subjected to any investigations while in any schooling institution
(e.g., suspensions, being expelled, subject of a complaint)? Yes☐ No☐
If yes, list ALL disciplinary or investigation records and the institution for each one.
EMPLOYMENT HISTORY
29. Starting with your current position and working chronologically backwards, list below your complete
employment history, including internships. Include each period of self-employment and/or any
periods of unemployment. If self-employed, state the activity in which you were engaged and
provide proof of income (e.g., tax returns, W-2 wage statements, 1099 miscellaneous income
statements). If there is a period of unemployment, indicate the reason and any source(s) of
income during that period (e.g., unemployment insurance, severance pay, savings, public
assistance).
Note: Include any previous employment with the City of New York that you may have had at any
time.
Page 44 of 107
Additional Space
Page 45 of 107
Employer
Title
Location of Job (Physical
Address)
Dates of Employment,
Self- Employment or
Unemployment (Month/Year)
Supervisor Name and Title
Supervisor Contact Information
From:
To:
Name:
Title:
Phone:
Email:
Employer and HR Contact
Information
Reason for Leaving
Phone:
Email:
Employer
Title
Location of Job (Physical
Address)
Dates of Employment,
Self- Employment or
Unemployment (Month/Year)
Supervisor Name and Title
Supervisor Contact Information
From:
To:
Name:
Title:
Phone:
Email:
Employer and HR Contact
Information
Reason for Leaving
Phone:
Email:
Include your base annual salary from current job: $
Page 46 of 107
Additional Space
Page 47 of 107
Employer
Title
Location of Job (Physical
Address)
Dates of Employment,
Self- Employment or
Unemployment (Month/Year)
Supervisor Name and Title
Supervisor Contact Information
From:
To:
Name:
Title:
Phone:
Email:
Employer and HR Contact
Information
Reason for Leaving
Phone:
Email:
Employer
Title
Location of Job (Physical
Address)
Dates of Employment,
Self- Employment or
Unemployment (Month/Year)
Supervisor Name and Title
Supervisor Contact Information
From:
To:
Name:
Title:
Phone:
Email:
Employer and HR Contact
Information
Reason for Leaving
Phone:
Email:
Page 48 of 107
Additional Space
Page 49 of 107
Employer
Title
Location of Job (Physical
Address)
Dates of Employment,
Self- Employment or
Unemployment (Month/Year)
Supervisor Name and Title
Supervisor Contact Information
From:
To:
Name:
Title:
Phone:
Email:
Employer and HR Contact
Information
Reason for Leaving
Phone:
Email:
Employer
Title
Location of Job (Physical
Address)
Dates of Employment,
Self- Employment or
Unemployment (Month/Year)
Supervisor Name and Title
Supervisor Contact Information
From:
To:
Name:
Title:
Phone:
Email:
Employer and HR Contact
Information
Reason for Leaving
Phone:
Email:
Page 50 of 107
Additional Space
Page 51 of 107
Employer
Title
Location of Job (Physical
Address)
Dates of Employment,
Self- Employment or
Unemployment (Month/Year)
Supervisor Name and Title
Supervisor Contact Information
From:
To:
Name:
Title:
Phone:
Email:
Employer and HR Contact
Information
Reason for Leaving
Phone:
Email:
Employer
Title
Location of Job (Physical
Address)
Dates of Employment,
Self- Employment or
Unemployment (Month/Year)
Supervisor Name and Title
Supervisor Contact Information
From:
To:
Name:
Title:
Phone:
Email:
Employer and HR Contact
Information
Reason for Leaving
Phone:
Email:

Page 52 of 107
Additional Space
Page 53 of 107
30A. Have you ever been disciplined, in any manner, in connection with any employment
(e.g., suspended, demoted, reprimanded, fined, penalized or terminated)? Yes☐ No☐
30B. Have you ever resigned from any employment while any charge or disciplinary action was
pending against you? Yes☐ No☐
30C. Have you ever been asked to resign from any employment? Yes☐ No☐
30D. Have you ever resigned from any employment to avoid being fired or disciplined, or after having
been told that you would be fired or disciplined? Yes☐ No☐
Page 54 of 107
Additional Space
Page 55 of 107
Dates you received
unemployment benefits
Reason for receiving unemployment benefits
From:
To:
From:
To:
From:
To:
Branch of Military
Type of Service (Active Duty or
National Guard/Reserve)
Final/Current Rank
Date Entered
Date Discharged
Type of Discharge
MILITARY SERVICE
31. Have you ever received unemployment benefits? Yes☐ No☐
If yes, provide the dates when you received them and the reason.
32. Have you ever served in any branch of the Armed Forces of the United States? Yes☐ No☐
If yes, provide the following information:
33. Have you ever been dishonorably discharge? Yes☐ No☐
34. Are you a disabled Veteran? Yes☐ No☐
35. Do you have any other military service to add (e.g., out of country military service?
Yes☐ No☐
If yes, please provide the same information as Question 32A on the back of this page.
Page 56 of 107
Additional Space
Page 57 of 107
Discipline Explanation
Failure to Complete the Full-Term Explanation
36A. While serving, were you ever the subject of any disciplinary action such as a Courts-Martial or
Non-Judicial Punishment? (e.g., Article 15, NJP, Navy/Marine Corps – “Captains Mast”, Air Force
– “Office Hours”) Yes☐ No☐
36B. If yes, provide an explanation of the discipline including the incident type, dates of the incident,
location of it, what discipline was received and such.
37A. While serving, did you ever fail to complete the full term of your military enlistment and/or
military service? Yes☐ No☐
37B. If yes, please explain the reason for failing to complete the full term of the enlistment/service.
Page 58 of 107
Additional Space
Page 59 of 107
If you answered yes to any of the above for Question 39, please provide the following information
on the next page and, if necessary, on the back of that same page.
38A. Did you register with the Selective Service? Yes ☐ No ☐ NA ☐
38B. If no, provide details as to why not below:
CIVIL AND CRIMINAL
INVESTIGATION HISTORY
Note: Offenses include felonies, misdemeanors, violations and all criminal court summons. A guilty
plea, guilty verdict, or plea of nolo contendere is a conviction even if, upon sentencing, you were never
imprisoned, only paid a fine, were conditionally or unconditionally discharged, or received a Certificate
of Relief from Disabilities. You MUST disclose any material sealed, expunged, or set aside under Federal
or State law, or any juvenile delinquent or youthful offender adjudications. You are not considered a
youthful offender simply because of your age at the time of the offense. Only a specific court finding
determines youthful offender status. If you are unsure whether you were determined to be a youthful
offender, list the offense(s) below and provide details.
39B. Have you ever been arrested for an offense in any jurisdiction in your lifetime? You must
include all offenses, including any offense involving driving while intoxicated or while ability is
impaired (or the equivalent in other states), an issue of a court appearance ticket or criminal
summons. Yes☐ No☐
39A. Have you ever been taken into custody or detained by law enforcement in any jurisdiction in
your lifetime, that did not result in an arrest? Yes☐ No☐
39C. Have you ever been questioned or interviewed by law enforcement in regard to any
incident/crime, even if you were not considered a suspect? Yes☐ No☐
Page 60 of 107
Additional Space
Page 61 of 107
1. Date of
Occurrence
Incident Type
Incident Location
(City/State)
Law Enforcement Agency
Status/Conviction/Final Disposition
Court of Conviction (Name and Location)
Additional Information (e.g., details on incident, involved parties)
2. Date of
Occurrence
Incident Type
Incident Location
(City/State)
Law Enforcement Agency
Status/Conviction/Final Disposition
Court of Conviction (Name and Location)
Additional Information (e.g., details on incident, involved parties)
3. Date of
Occurrence
Incident Type
Incident Location
(City/State)
Law Enforcement Agency
Status/Conviction/Final Disposition
Court of Conviction (Name and Location)
Additional Information (e.g., details on incident, involved parties)
Page 62 of 107
Additional Space
Page 63 of 107
40A. Are you currently on probation?
40B. Are you currently on parole or supervised release?
If Yes to 40 or 40B, provide details, including dates, below:
Yes☐ No☐
Yes☐ No☐
42. Have you ever been named, for any reason, or referred to in (including as an unindicted co
-conspirator), any indictment or other accusatory instrument, or been named in or the subject
of, a search warrant or court-ordered electronic surveillance?
If Yes, provide details, including dates, below:
Yes☐ No☐
43. Have you been arrested, charged, or indicted in connection with any criminal matter which is
stilling pending in court?
Yes☐ No☐
If yes, provide the following information:
44A. Have you ever been subpoenaed, called as a witness, questioned or interviewed, or asked to
provide testimony or documents before any federal, state, or local prosecutor, court
legislative, civil, regulatory, or criminal investigate body (including DOI and its Inspector
General), or grand jury? Yes☐ No☐
Page 64 of 107
Additional Space
Page 65 of 107
If you were granted immunity, in any form, or entered into a consent decree, in any of the above
matter(s), please explain:
45A. Have you ever asserted the Fifth Amendment right against self-incrimination or refused to
testify before any federal, state, or local prosecutor, court legislative, civil, regulatory, or
criminal investigate body (including DOI and its Inspector General), or grand jury, or been cited
for contempt of any court, legislative, civil, or criminal investigative body, or grand jury?
Yes☐ No☐
45B. If yes, provide the following information:
46A. Have you been informed, or do you have reason to believe, that you are under
investigation by any federal, state, or local prosecutor, legislative, civil, or criminal
investigate body (including DOI and its Inspector General), or grand jury? Yes☐ No☐
46B. If yes, provide the following information:
44B. If you answered yes to Question 44A, provide the following information.
Page 66 of 107
Additional Space
Page 67 of 107
Date Order Issued
Date Order Expired
Court that Issued
the Order
Docket/Case Number
Explanation of the Order (e.g., brief narrative, parties involved, any results/outcomes)
Date Order Issued
Date Order Expired
Court that Issued
the Order
Docket/Case Number
Explanation of the Order (e.g., brief narrative, parties involved, any results/outcomes)
47A. Have you been informed, or do you have reason to believe, that you currently are, or have
previously been, the subject of an investigation, or of a complaint filed, which alleged child
abuse or domestic violence? Yes☐ No☐
47B. Has a Family Court or any other lawful authority ever rendered a finding indicating that
you have abused or neglected a child? Yes☐ No☐
If Yes to 24A and 24B, provide details, including dates, below:
48. Have you ever been a defendant, plaintiff, protected party, respondent, or the like, on any
Order of Protection, Restraining Order or similar document of that nature?
If Yes, provide an explanation below: Yes☐ No☐
Page 68 of 107
Additional Space
Page 69 of 107
1. Date
Commenced
Title of Action
Role
Jurisdiction
Status/Disposition
Additional Information (details of the case, involved parties, and such)
2. Date
Commenced
Title of Action
Role
Jurisdiction
Status/Disposition
Additional Information (details of the case, involved parties, and such)
3. Date
Commenced
Title of Action
Role
Jurisdiction
Status/Disposition
Additional Information (details of the case, involved parties, and such)
49. Have you ever knowingly associated with any person known or reputed to be a member or
associate of an organized crime group and/or gang? Yes☐ No☐
If Yes, provide details, including the identity of the person and the nature and dates of your
association, below:
50. Have you been involved as a party to any civil litigation, administrative action,
administrative proceeding or legal action (includes divorce proceedings)? Yes☐ No☐
If yes, provide the following information (additions can be made to the back of this page:
Page 70 of 107
Additional Space
Page 71 of 107
51. Have you ever been informed of an overpayment of, or requested or required to repay any
federal, state, or local government-issued benefit or payment (e.g., Public Assistance, Food
Stamps, Unemployment Insurance, Workers Compensation, Medicaid, Social Security, public
pension, public housing/Section 8 rent subsidy, etc.)?
Yes☐ No☐
If Yes, provide details, including dates and the reason(s) for the repayment/recoupment,
below:
TAX INFORMATION AND
FINANCIAL STATUS
Note: Review your tax records and provide precise filing information. This
Department verifies with the tax authorities whether tax returns were filed and
the dates of filing. Copies of your tax returns must be provided upon request.
Candidates undergoing a background investigation who were required by law to
file a federal and/or state income tax return for a previous year, and who have not
filed as of yet MUST file all outstanding tax returns. To avoid delaying the
completion of your background investigation, promptly file any outstanding
return(s) IN PERSON and attach to this questionnaire a copy of the return(s),
stamped as having been received by the tax authority as proof of filing.
Question 52 applies to EVERY year within the past ten (10) years. “Due date”
means April 15
th
of the following year, or other date established by governing
statute. Properly obtained extension is an extension period granted by the tax
authority upon filing a timely application in accordance with applicable law and/or
regulations.
52. Have you filed your federal and state income tax returns by the due date or within a
properly obtained extension period for each of the past ten (10) years?
Page 72 of 107
Additional Space
Page 73 of 107
If you answered no to Question 52, provide the following information:
During the past ten (10) years, if you have NOT filed a return for any year or have not filed a return
for any year by the due date or within a properly obtained extension period, provide the
information requested below. If you were not required to file (e.g., you were unemployed or
earned less than the amount required for filing), state so below.
The year(s) in which you did not file, or did not file by the due date or within a properly obtained
extension period, indicate whether you are referring to your federal or state returns, or to both:
The address(es) where you lived during the year(s) in question:
The date(s), if any, when you filed each year’s return:
The reason(s) for the late or non-filing:
Any interest or penalties assessed for the year(s) in question:
Were you due a refund or did you owe money for the year(s) in question? If you owed money,
state the amount(s):
Note: Attach to this questionnaire a copy of any statement of settlement, consent decree, or other
dispositive document issued by the tax authority regarding the above return(s).
53. Has any tax return filed by you been the subject of an audit by any tax authority within the past
ten (10) years? Yes☐ No☐
If yes, give details, including findings of audit and any interest or penalties assessed and/or paid.
In addition, attach to this questionnaire a copy of the tax authority’s findings.

Page 74 of 107
Additional Space
Page 75 of 107
Tax Year
Street Address, Apt. Number, City, State, Zip Code
54. Provide the address(es) of the tax residence(s) you reported on your return(s) for the past ten
(10) years:
55. Have you ever filed a petition under any chapter of bankruptcy code, or has been the subject of
a bankruptcy or reorganization proceeding, either personally or on behalf of a business?
Yes☐ No☐
56. Have you ever had any loan defaulted or had property repossessed and/or foreclosed?
Yes☐ No☐
57. Have you ever had any type of lien placed against you personally or on a business you own?
Yes☐ No☐
58. Have you ever been contacted by any collections agency for any debts owed or delinquent
accounts? Yes☐ No☐
59. Have you ever had any judgments filed against you or had your wages garnished?
Yes☐ No☐
If you answered yes to any question from Question 55 to 59, provide copies of any and all
paperwork regarding that issue, such as the bankruptcy discharge documents (including a list
of creditors), any mail, letters, statements and/or files, with your background paperwork.
Page 76 of 107
Additional Space
Page 77 of 107
Name of
Filer/Agency
Name of Court
Date Filed
Month / Day /
Year
Date
Discharged
Month / Day /
Year
Total Debt Discharged
Detailed Explanation
(e.g., reason for bankruptcy, type of loan or lien, type of judgment, what was foreclosed, etc.)
Name of
Filer/Agency
Name of Court
Date Filed
Month / Day /
Year
Date
Discharged
Month / Day /
Year
Total Debt Discharged
Detailed Explanation
(e.g., reason for bankruptcy, type of loan or lien, type of judgment, what was foreclosed, etc.)
60. If you answered yes to any question from question 55 to 59, provide the following
information, when applicable.
Bankruptcy petition type: Chapter 7 ☐ Chapter 11 ☐ Chapter 13 ☐ N/A ☐
Please provide the following information regarding any bank accounts, mortgages
and/or current loan:
Page 78 of 107
Additional Space
Page 79 of 107
Name of Bank or
Financial Institution
Address
Phone Number
Name of Bank or
Financial Institution
Address
Phone Number
Name of Lender
Address
Phone Number
Name of Lender
Address
Phone Number
Type of Loan and
Name of Lender
Address
Phone Number
Type of Loan and
Name of Lender
Address
Phone Number
Type of Loan and
Name of Lender
Address
Phone Number
Please provide the following information regarding any bank accounts, mortgages and/or
current loans.
61A. Do you have any bank checking accounts? Yes☐ No☐
61B. Do you have any mortgages? Yes☐ No☐
61C. Do you have any loans (including student, vehicle or any other)? Yes☐ No☐
Page 80 of 107
Additional Space

Page 81 of 107
Position/Title
Exam and List Number
(if applicable)
Date
Applied/Taken
Status
Exam Number:
List Number:
Exam Number:
List Number:
1. Agency Name
Exam Number
List Number
Date Applied/Taken
Background Investigation (Y/N)
Status of Application
2. Agency Name
Exam Number
List Number
Date Applied/Taken
Background Investigation (Y/N)
Status of Application
3. Agency Name
Exam Number
List Number
Date Applied/Taken
Background Investigation (Y/N)
Status of Application
APPLICATIONS TO GOVERNMENT AGENCIES
62. Have you ever previously applied to the NYC Department of Finance for any position, including
any position with the NYC Office of the Sheriff? Yes☐ No☐
If yes, provide the following information:
63. Have you ever, in your lifetime, applied to any other law enforcement agency, within or outside
of New York City? Yes☐ No☐
If yes, provide the following information:
Page 82 of 107
Additional Space
Page 83 of 107
4. Agency Name
Exam Number
List Number
Date Applied/Taken
Background Investigation (Y/N)
Status of Application
5. Agency Name
Exam Number
List Number
Date Applied/Taken
Background Investigation (Y/N)
Status of Application
1. Agency Name
Exam Number
List Number
Date Applied/Taken
Background Investigation (Y/N)
Status of Application
2. Agency Name
Exam Number
List Number
Date Applied/Taken
Background Investigation (Y/N)
Status of Application
3. Agency Name
Exam Number
List Number
Date Applied/Taken
Background Investigation (Y/N)
Status of Application
64. Have you ever, in your lifetime, applied to any other government agency for any title?
Yes☐ No☐
If yes, provide the following information:
Page 84 of 107
Additional Space
Page 85 of 107
4. Agency Name
Exam Number
List Number
Date Applied/Taken
Background Investigation (Y/N)
Status of Application
5. Agency Name
Exam Number
List Number
Date Applied/Taken
Background Investigation (Y/N)
Status of Application
Date
Agency
Position
Reason for Bar or Disqualification (Full Details)
Date
Agency
Position
Reason for Bar or Disqualification (Full Details)
Date
Agency
Position
Reason for Bar or Disqualification (Full Details)
65. Have you ever been barred or disqualified from appointment or employment to a position with
any government agency in any civil service position? Yes☐ No☐
If yes, provide the following information:
Page 86 of 107
Additional Space
Page 87 of 107
Make
Model
Caliber
Serial Number
Issuing
Body
License/Permit #/
Type
Basis for License/
Permit
Date Issued
Date Expires
FIREARMS LICENSES
AND PERMITS
66A. Do you have a license or permit to possess or carry a firearm? Yes☐ No☐
If yes, provide the following information and attach to this questionnaire a copy of the license
or permit:
66B. If yes to Question 66A, state the agency that conducted your background investigation:
67. Do you own any firearms? Yes☐ No☐
If yes, indicate amount and provide the following information:
Page 88 of 107
Additional Space
Page 89 of 107
Date of Revocation,
Suspension or Denial
Month / Day / Year
Issuing Body
Reason or Basis for Revocation,
Suspension or Denial
68A. Have you ever applied for a pistol license/permit, dealer’s license or gunsmith license but was
disapproved? Yes☐ No☐
68B. Have you ever had a pistol license/permit, dealer’s license or gunsmith license revoked or
suspended? Yes☐ No☐
If yes to Question 68A or 68B, provide the following information:
Page 90 of 107
Additional Space
Page 91 of 107
MISCELLANEOUS
69. Have you ever been fingerprinted for any reason other than for a Civil Service Examination or
application to a government agency? Yes☐ No☐
If yes, provide details below:
71A. Are you currently using or experimenting with, in any way or form, any type of drugs, narcotics,
or controlled substances, including marijuana and its derivatives (not prescribed by your
doctor)? Yes☐ No☐
70. Have you ever taken a polygraph test, also known as a lie detector test? Yes☐ No☐
If yes, provide details below:
71B. Have you ever used or experimented with, in any way or form, any type of drugs, narcotics,
or controlled substances, including marijuana and its derivatives (not prescribed by your
doctor? Yes☐ No☐
If you answered yes to Question 71A or 71B, provide details:
Dates of usage
Types of Substance
Amounts used and Reason
Page 92 of 107
Additional Space
Page 93 of 107
71C. Have you ever sold, gave away or profited from selling any type of unlawful controlled substance
in any state or Federal Statute? Yes☐ No☐
If yes, provide details:
Dates sold
Types of Substance(s) sold
Where it was sold
71D. If you answered yes to any question from Question 71A to 71C, were you ever arrested or given
a summons regarding the controlled substances? Yes☐ No☐
If yes, explain:
72A. Have you ever abused alcohol? Yes☐ No☐
72B. Have you ever been arrested or issued a summons for an alcohol related incident?
Yes☐ No☐
If yes, explain:
Page 94 of 107
Additional Space
Page 95 of 107
Bond/Surety Agency
Date
Month / Year
Reason Refused or Denied, Revoked or
Suspended
72A. Have you ever engaged in any type or form of illegal gambling activities? Yes☐ No☐
72B. Have you ever been arrested or issued a summons for illegal gambling related incidents?
Yes☐ No☐
If yes, explain:
73. Have you ever been refused or denied a bond or surety, or had a bond or surety revoked or
suspended? Yes☐ No☐
If yes, provide the following information:
74. Are you proficient in another language or languages? Yes☐ No☐
If yes, indicate language(s):
75. Is there any fact, issue, or other circumstance not covered in this background questionnaire,
which you feel may be relevant to your fitness to perform the duties of the position for which
your background is being investigated?
If yes, explain below:
Page 96 of 107
Additional Space
Page 97 of 107
Conflicts of Interest
76. Are there any matters which may involve a conflict of interest in connection with your
appointment to the position for which you are being considered which are not fully
covered by your answers to this questionnaire? This includes owning or being employed by
a business or organization that is contracted with DOF and/or the New York City Sheriff’s
Office and/or having family or relatives that are employed with DOF and/or the New York
City Sheriff’s Office?
If Yes, state below the pertinent facts:
Additional Remarks
77. Are there any comments you wish to make or information you would like to add?
Page 98 of 107
Additional Space
Page 99 of 107
41. Please provide a brief summary on why you would like to be a Sheriff Investigator or
Deputy Sheriff:
Page 100 of 107
CERTIFICATION AND SIGNATURE
THIS QUESTIONNAIRE MUST BE SIGNED AND SWORN TO BY YOU
BEFORE A NOTARY PUBLIC OR COMMISSIONER OF DEEDS
I, ________________________________________, being duly sworn, state that I have read and
understand all the questions and answers contained in the foregoing pages of this questionnaire and
the _________ page(s) of the addendum which I have appended thereto; that I have supplied full and
complete information in answer to each question therein to the best of my knowledge, information,
and belief; and that all the information supplied therein is true.
I further understand that a false statement or intentional omission made in this questionnaire or in
connection with this background investigation may result in the imposition of disciplinary penalties,
including termination of employment, or disqualification from future employment and, in addition,
may subject me to criminal prosecution.
__________________________________
Signature
Subscribed and sworn to before me
this_________day of____________20____
___________________________________
Notary Public or Commissioners of Deeds
THIS BACKGROUND INVESTIGATION QUESTIONNAIRE IS
NOT A PUBLIC DOCUMENT
Page 101 of 107
EXAM NO.
LIST NO.
From:
To: Deputy Cadet Processing
Subject: FIREARM SECURITY
1. I realize that as a Deputy Sheriff/Investigator, I will be responsible for securing
my weapon(s). I will follow the instructions/training given to me at the Sheriff’s Office Law
Enforcement Academy as to the proper procedure to use to secure my weapon(s).
2. The following member(s) of my family and/or any other person(s) who reside in my
household, whether or not related to me, have been arrested for the charges listed below.
(use additional form if more space is needed)
3. The above is all the knowledge I have concerning my family and
household members’ arrest record(s).
Signature
Date
FIREARM SECURITY FORM
Page 102 of 107
Page 103 of 107
INQUIRY REGRADING CONVICTIONS FOR
MISDEMEANOR CRIMES OFDOMESTIC VIOLENCE
Pursuant to Title 18 U.S.C. Section 922 (g) (9)
The purpose of this form is to obtain information that will assist the New York City Sheriff’s Office in
determining whether any of its applicants have been adversely affected by federal law, title 18 U.S.C. Section 922
(g) (9). You are directed to complete this form and return it, within ten (10) working days of your receipt of the
form, to your Character Assessment Section Investigator. Failure to complete this form truthfully and within ten
(10) days of receipt may result in your disqualification.
Applicants may seek the advice of counsel prior to responding to the questions contained in this form.
However, the form must be completed, notarized, and submitted to your investigator within ten (10) days of
receipt. The New York City Sheriff’s Office will notify the Licensing agency and/or appropriate authorities when
informed of an applicant who reports the possession of firearms or ammunition in violation of this law.
1. Have you ever been convicted of a Misdemeanor Crime of Domestic Violence, in any court, anywhere,
including a military tribunal? Indicate: YES NO
A "Misdemeanor Crime of Domestic Violence" is defined by 18 U.S.C. 921 (a) (33) (A) as follows: An
offense that (i) is a misdemeanor under federal or state law and (ii) has as an element, the use or attempted use
of physical force or the threatened use of a deadly weapon, committed by:
a.- A current or former spouse, parent or guardian of the victim.
b.- A person with whom the victim shares a child in common.
c.- A person who was or is cohabiting with the victim as a spouse, parent or guardian.
d.- A person similarly situated to a spouse, parent or guardian of the victim.
2. If you answered "yes" to question 1, provide the following information with respect to the conviction:
Court/Jurisdiction
Docket/Case#
Statute/Charge
Date Sentenced
If you answered "yes" to question No.1:
a. Were you pardoned? Indicate: YES NO
b. Was your conviction expunged? Indicate: YES NO
c. If any of your civil rights were removed as a result of your conviction, have all of your rights been
restored? Indicate: N/A YES NO
3. If you answered "Yes" to question 2a, b or c attach copies of documents verifying your response.
I hereby attest that all of the statements herein are true under the penalty of perjury and its related offenses
pursuant to section 210 of the Penal Law.
Name Exam No.
List No. Position Sought S.S. No.
Date Signature
Sworn to before me this day of , 20
Notary
Public
DOMESTIC VIOLENCE INQUIRY
Page 104 of 107
Page 105 of 107
Candidates Name: ____________________________________________
Exam No. ____________ List No. __________
You are now a candidate for the position of Deputy Sheriff/ Investigator with the
New York City Finance Department, Office of the City Sheriff. You must keep the
Character Assessment Section Investigator assigned to your case fully informed of any
events in your life which may have an impact upon your character or suitability for
appointment as a Deputy Sheriff/Investigator, to fully investigate your background and
history.
You must notify your investigator with any events or changes in your life
including, but not limited to: change of address; change of phone number; change of
employment; change of marital status; whether you have received any summonses
(traffic, criminal, or civil), been arrested, or been involved in any way with any police
department or law enforcement agency as a witness to, victim of, or suspect in any
crime or violation of law. You will also be required to be screened for social media to
ensure that you comply with the agency social media policy.
FAILURE TO PROMPTLY INFORM YOUR INVESTIGATOR OF ANY SUCH
CHANGES OR EVENTS MAY RESULT IN YOUR DISQUALIFICATION FOR
EMPLOYMENT AS A DEPUTY SHERIFF/INVESTIGATOR.
I understand my obligation to inform the New York City Department of Finance
Office of the City Sheriff’s Character Assessment Section of any events or changes in
my life as described above as well as be willingly to allow the Sheriffs Character
Assessment Section to screen any and all social media accounts that belong to me in
compliance with Social media policy. I understand that my failure to promptly inform my
investigator of any such changes or events may result in disqualification for employment
as a Deputy Sheriff/ Investigator.
____________________________
Date Signature of Candidate
Notice to Deputy Sheriff/Investigator Candidates
Page 106 of 107

Page 107 of 107
NY0300000 __________________________
Deputy Cadet Processing Date
3010 Starr Avenue
Queens, NY 11101
Tel: (718) 707-2122
Fax: (718) 707-2190
Exam No. ______________________ List No. ________________
I, ___________________________________________________, do hereby authorize the Veterans Agencies;
United States Army; Navy; Air Force; Marines; Coast Guard; Military Reserves; all Law Enforcement
Agencies, City, State, and Federal Tax Bureaus; Welfare and Unemployment Services; Credit Bureaus;
Schools; Universities, Physicians, Hospitals and Institutions; all State, City and County Civil Service
Commissions; and all Federal, State, City and Local Courts, including those records relating to Youthful
Offender Adjudication, including those pursuant to NYS CPL § 720.35; to furnish the New York City Sheriff’s
Office with any and all available information and copies of records as well as current and past civil service
standings and the outcome of any investigations ongoing or discontinued regarding me. This information will
be used to determine my suitability for possible appointment as Deputy Sheriff or Investigator with New York
City Sheriff’s Office.
I authorize the New York City Sheriff’s Office to make inquiry of my present and past employers regarding
my character, integrity and reputation. (Make note if you do not wish to have your present employer contacted
and provide an explanation below.)
I acknowledge by this authorization that I release you from any obligations or liability in the disclosure
of the contents of such files and the professional observations or opinions contained therein.
Yes, you may contact my present employer.
No, I do not want my present employer contacted.
Explain: ___________________________________________________________________________
Note: A photocopy of this authorization shall be considered as effective and valid as the original.
________________________________ ________________________________
Signature of Applicant Print Name
Sworn to me this ________________
day of ________________, 20_____
______________________________
Notary Public
AUTHORIZATION FOR RELEASE OF INFORMATION
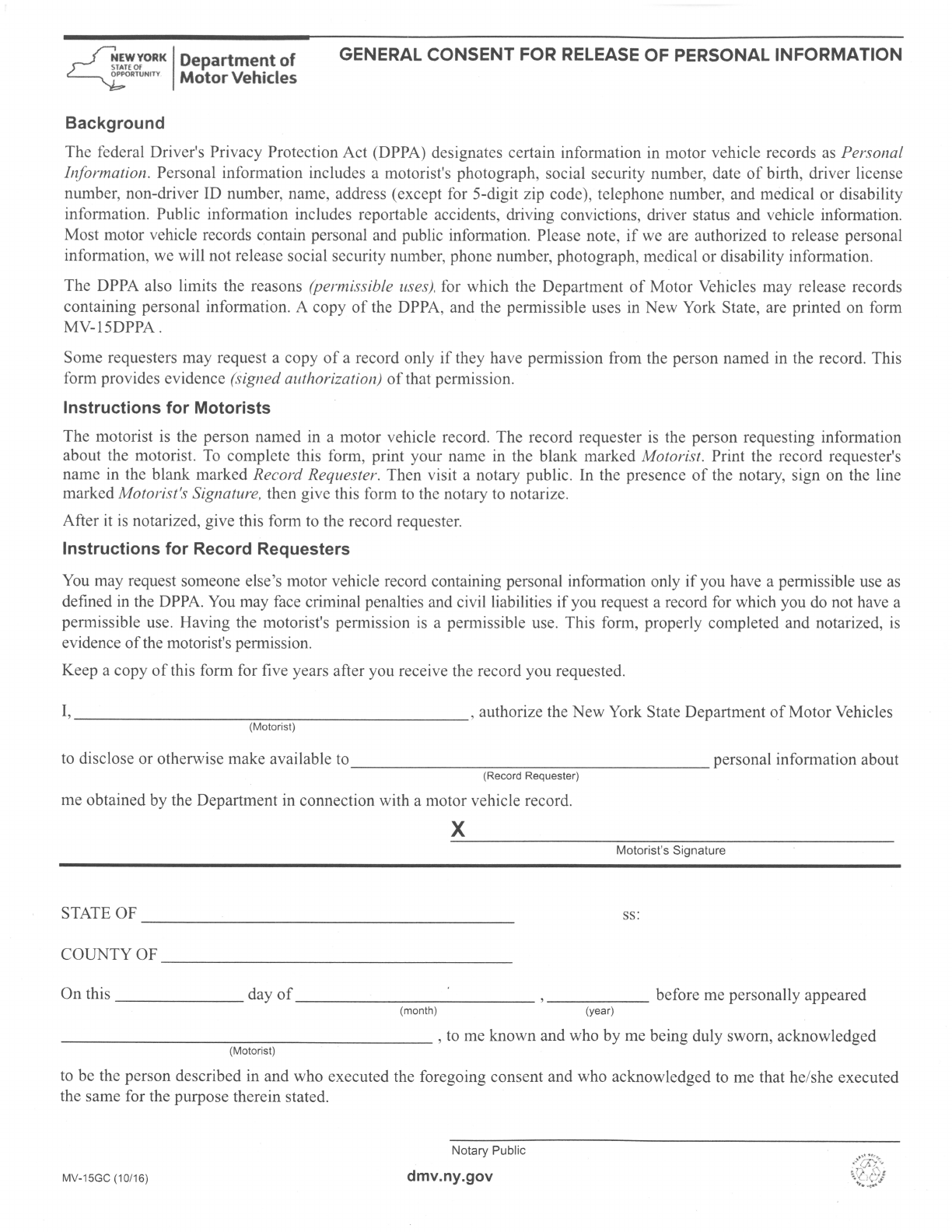
INSTRUCTION AND INFORMATION SHEET FOR SF 180, REQUEST PERTAINING TO MILITARY RECORDS
1. General Information. The Standard Form 180, Request Pertaining to Military Records (SF180) is used to request information from military records.
Certain identifying information is necessary to determine the location of an individual's record of military service. Please try to answer each item on the SF
180. If you do not have and cannot obtain the information for an item, show "NA," meaning the information is "not available". Include as much of the
requested information as you can. Incomplete information may delay response time. To determine where to mail this request see Page 2 of the SF180 for
record locations and facility addresses.
Online requests may be submitted to the National Personnel Records Center (NPRC) by a veteran or deceased veteran’s next-of-kin using eVetRecs at
http://www.archives.gov/veterans/military-service-records/ .
2. Personnel Records/Military Human Resource Records/Official Military Personnel File (OMPF) and Medical Records/Service Treatment
Records (STR). Personnel records of military members who were discharged, retired, or died in service LESS THAN 62 YEARS AGO and medical
records are in the legal custody of the military service department and are administered in accordance with rules issued by the Department of Defense and
the Department of Homeland Security (DHS, Coast Guard). STRs of persons on active duty are generally kept at the local servicing clinic. After the last
day of active duty, STRs should be requested from the appropriate address on page 2 of the SF 180. (See item 3, Archival Records, if the military member
was discharged, retired or died in service more than 62 years ago.)
a. Release of information: Release of information is subject to restrictions imposed by the military services consistent with Department of Defense
regulations, the provisions of the Freedom of Information Act (FOIA) and the Privacy Act of 1974. The service member (either past or present) or
the member's legal guardian has access to almost any information contained in that member's own record. The authorization signature of the service
member or the member's legal guardian is needed in Section III of the SF180. Others requesting information from military personnel records and/or
STRs must have the release authorization in Section III of the SF 180 signed by the member or legal guardian. If the appropriate signature cannot be
obtained, only limited types of information can be provided. If the former member is deceased, the surviving next-of-kin may, under certain
circumstances, be entitled to greater access to a deceased veteran's records than a member of the general public. The next-of-kin may be any of the
following: unremarried surviving spouse, father, mother, son, daughter, sister, or brother. Requesters MUST provide proof of death, such as a
copy of a death certificate, newspaper article (obituary) or death notice, coroner’s report of death, funeral director’s signed statement of
death, or verdict of coroner’s jury.
b. Fees for records: There is no charge for most services provided to service members or next-of-kin of deceased veterans. A nominal fee is
charged for certain types of service. In most instances, service fees cannot be determined in advance. If your request involves a service fee, you will
receive an invoice with your records.
3. Archival Records. Personnel records of military members who were discharged, retired, or died in service 62 OR MORE YEARS AGO have been
transferred to the legal custody of NARA and are referred to as “archival records”.
a. Release of Information: Archival records are open to the public. The Privacy Act of 1974 does not apply to archival records, therefore, written
authorization from the veteran or next-of-kin is not required. In order to protect the privacy of the veteran, his/her family, and third parties named in
the records, the personal privacy exemption of the Freedom of Information Act (5 U.S.C. 552 (b) (6)) may still apply and may preclude the release
of some information.
b. Fees for Archival Records: Access to archival records are granted by offering copies of the records for a fee (44 U.S.C. 2116 (c)). If a fee applies
to the photocopies of documents in the requested record, you will receive an invoice. Photocopies will be sent after payment is made. For more
information see http://www.archives.gov/st-louis/archival-programs/military-personnel-archival/ompf-archival-requests.html.
4. Where reply may be sent. The reply may be sent to the service member or any other address designated by the service member or other authorized
requester. If the designated address is NOT registered to the addressee by the U.S. Postal Service (USPS), provide BOTH the addressee’s name AND “in
care of” (c/o) the name of the person to whom the address is registered on the NAME line in Section III, item 3, on page 1 of the SF 180. The COMPLETE
address must be provided, INCLUDING any apartment/suite/unit/lot/space/etc. number.
5. Definitions and abbreviations. DISCHARGED -- the individual has no current military status; SERVICE TREATMENT RECORD (STR) -- The
chronology of medical, mental health, and dental care received by service members during the course of their military career (does not include records of
treatment while hospitalized); TDRL – Temporary Disability Retired List.
6. Service completed before World War I. National Archives Trust Fund (NATF) forms must be used to request these records. Obtain the forms by e-
mail from [email protected] or write to the Code 6 address on page 2 of the SF 180.
PRIVACY ACT OF 1974 COMPLIANCE INFORMATION
The following information is provided in accordance with 5 U.S.C. 552a(e)(3) and applies to this form. Authority for collection of the information is 44
U.S.C. 2907, 3101, and 3103, and Public Law 104-134 (April 26, 1996), as amended in title 31, section 7701. Disclosure of the information is voluntary. If
the requested information is not provided, it may delay servicing your inquiry because the facility servicing the service member's record may not have all of
the information needed to locate it. The purpose of the information on this form is to assist the facility servicing the records (see the address list) in locating
the correct military service record(s) or information to answer your inquiry. This form is then retained as a record of disclosure. The form may also be
disclosed to Department of Defense components, the Department of Veterans Affairs, the Department of Homeland Security (DHS, U.S. Coast Guard), or
the National Archives and Records Administration when the original custodian of the military health and personnel records transfers all or part of those
records to that agency. If the service member was a member of the National Guard, the form may also be disclosed to the Adjutant General of the
appropriate state, District of Columbia, or Puerto Rico, where he or she served.
PAPERWORK REDUCTION ACT PUBLIC BURDEN STATEMENT
Public burden reporting for this collection of information is estimated to be five minutes per request, including time for reviewing instructions and
completing and reviewing the collection of information. Send comments regarding the burden estimate or any other aspect of the collection of information,
including suggestions for reducing this burden, to National Archives and Records Administration (ISSD), 8601 Adelphi Road, College Park, MD 20740-
6001. DO NOT SEND COMPLETED FORMS TO THIS ADDRESS. SEND COMPLETED FORMS TO THE APPROPRIATE ADDRESS LISTED ON
PAGE 2 OF THE SF 180.
Standard Form 180 (Rev. 11/2015) (Page 1) Authorized for local reproduction
Prescribed by NARA (36 CFR 1233.18 (d)) Previous edition unusable OMB No. 3095-0029 Expires 04/30/2018
REQUEST PERTAINING TO MILITARY RECORDS
Requests from veterans or deceased veteran’s next-of-kin may be submitted online by using eVetRecs at http://www.archives.gov/veterans/military-service-records/
To ensure the best possible service, please thoroughly review the accompanying instructions before filling out this form. PLEASE PRINT LEGIBLY OR TYPE BELOW.
SECTION I - INFORMATION NEEDED TO LOCATE RECORDS (Furnish as much information as possible.)
1. NAME USED DURING SERVICE (last, first, full middle)
2. SOCIAL SECURITY #
3. DATE OF BIRTH
4. PLACE OF BIRTH
5. SERVICE, PAST AND PRESENT (For an effective records search, it is important that ALL service be shown below.)
BRANCH OF SERVICE
DATE
ENTERED
DATE
RELEASED
OFFICER
ENLISTED
SERVICE NUMBER
(If unknown, write “unknown”)
a. ACTIVE
b. RESERVE
c. STATE
NATIONAL
GUARD
6. IS THIS PERSON DECEASED?
NO YES -
MUST provide Date of Death if veteran is deceased:
7. DID THIS PERSON RETIRE FROM MILITARY SERVICE?
NO YES
SECTION II – INFORMATION AND/OR DOCUMENTS REQUESTED
1. CHECK THE ITEM(S) YOU ARE REQUESTING:
DD Form 214 or equivalent. Year(s) in which form(s) issued to veteran:
This form contains information normally needed to verify military service. A copy may be sent to the veteran, the deceased veteran’s next-of-kin, or other
persons or organizations, if authorized in Section III, below. An UNDELETED DD214 is ordinarily required to determine eligibility for benefits. If you
request a DELETED copy, the following items will be blacked out: authority for separation, reason for separation, reenlistment eligibility code, separation
(SPD/SPN) code, and, for separations after June 30, 1979, character of separation and dates of time lost.
An UNDELETED copy will be sent UNLESS YOU SPECIFY A DELETED COPY by checking this box: I want a DELETED copy.
Medical Records Includes Service Treatment Records, Health (outpatient) and Dental Records. IF HOSPITALIZED (inpatient) the FACILITY NAME and
DATE (month and year) for EACH admission MUST be provided:
Other (Specify):
2. PURPOSE: (Providing information about the purpose of the request is strictly voluntary; however, it may help to provide the best possible response and may
result in a faster reply. Information provided will in no way be used to make a decision to deny the request.)
Benefits (explain)
Employment
VA Loan Programs
Medical
Genealogy
Correction
Personal
Other (explain)
EExplain here:
SECTION III - RETURN ADDRESS AND SIGNATURE
1. REQUESTER NAME:
2.
I am the MILITARY SERVICE MEMBER OR VETERAN identified in Section
I, above.
I am the VETERAN’S LEGAL GUARDIAN (MUST submit copy of Court
Appointment) or AUTHORIZED REPRESENTATIVE (MUST submit copy of
Authorization Letter or Power of Attorney)
I am the DECEASED VETERAN’S NEXT-OF-KIN (MUST submit Proof of
Death. See item 2a on instruction sheet.)
OTHER
(Relationship to deceased veteran)
(Specify type of Other)
3. SEND INFORMATION/DOCUMENTS TO:
(Please print or type. See item 4 on accompanying instructions.)
4. AUTHORIZATION SIGNATURE: I declare (or certify, verify, or
state) under penalty of perjury under the laws of the United States of
America that the information in this Section III is true and correct and
that I authorize the release of the requested information. (See items 2a or
3a on accompanying instruction sheet. Without the Authorization Signature
of the veteran, next-of-kin of deceased veteran, veteran’s legal guardian,
authorized government agent, or other authorized representative, only
limited information can be released unless the request is archival. No
signature is required if the request if for archival records. )
Name
Street Apt.
______________________________________________________________
City State Zip Code
*
This form is available at http://www.archives.gov/veterans/military-service-
records/standard-form-180.html on the National Archives and
Records Administration (NARA) web site. *
Signature Required - Do not print Date
Daytime phone
Fax Number
Email address
-
-
-
-
Standard Form 180 (Rev. 11/2015) (Page 2) Authorized for local reproduction
Prescribed by NARA (36 CFR 1233.18 (d)) Previous edition unusable OMB No. 3095-0029 Expires 04/30/2018
LOCATION OF MILITARY RECORDS
The various categories of military service records are described in the chart below. For each category there is a code number which indicates the address at the bottom of the
page to which this request should be sent. Please refer to the Instruction and Information Sheet accompanying this form as needed.
BRANCH
CURRENT STATUS OF SERVICE MEMBER
ADDRESS CODE
Personnel
Record
Medical or Service
Treatment Record
AIR
FORCE
Discharged, deceased, or retired before 5/1/1994
14
14
Discharged, deceased, or retired 5/1/1994 – 9/30/2004
14
11
Discharged, deceased, or retired 10/1/2004 – 12/31/2013
1
11
Discharged, deceased, or retired on or after 1/1/2014
1
13
Active (including National Guard on active duty in the Air Force), TDRL, or general officers retired with pay
1
Reserve, IRR, Retired Reserve in non-pay status, current National Guard officers not on active duty in the Air Force, or National Guard
released from active duty in the Air Force
2
Current National Guard enlisted not on active duty in the Air Force
2
13
COAST
GUARD
Discharge , deceased, or retired before 1/1/1898
6
Discharged, deceased, or retired 1/1/1898 – 3/31/1998
14
14
Discharged, deceased, or retired 4/1/1998 – 9/30/2006
14
11
Discharged, deceased, or retired 10/1/2006 – 9/30/2013
3
11
Discharged, deceased, or retired on or after 10/1/2013
3
14
Active, Reserve, Individual Ready Reserve or TDRL
3
MARINE
CORPS
Discharged, deceased, or retired before 1/1/1895
6
Discharged, deceased, or retired 1/1/1905 – 4/30/1994
14
14
Discharged, deceased, or retired 5/1/1994 – 12/31/1998
14
11
Discharged, deceased, or retired 1/1/1999 - 12/31/2013
4
11
Discharged, deceased, or retired on or after 1/1/2014
4
8
Individual Ready Reserve
5
Active, Selected Marine Corps Reserve, TDRL
4
ARMY
Discharged, deceased, or retired before 11/1/1912 (enlisted) or before 7/1/1917 (officer)
6
Discharged, deceased, or retired 11/1/1912 – 10/15/1992 (enlisted) or 7/1/1917 – 10/15/1992 (officer)
14
Discharged, deceased, or retired 10/16/1992 – 9/30/2002
14
11
Discharged, deceased, or retired (including TDRL) 10/1/2002 – 12/31/2013
7
11
Discharged, deceased, or retired (including TDRL) on or after 1/1/2014
7
9
Current Soldier (Active, Reserve (including Individual Ready Reserve) or National Guard)
7
NAVY
Discharged, deceased, or retired before 1/1/1886 (enlisted) or before 1/1/1903 (officer)
6
Discharged, deceased, or retired 1/1/1886 – 1/30/1994 (enlisted) or 1/1/1903 – 1/30/1994 (officer)
14
14
Discharged, deceased, or retired 1/31/1994 – 12/31/1994
14
11
Discharged, deceased, or retired 1/1/1995 – 12/31/2013
10
11
Discharged, deceased, or retired on or after 1/1/2014
10
8
Active, Reserve, or TDRL
10
PHS
Public Health Service - Commissioned Corps officers only
12
ADDRESS LIST OF CUSTODIANS and SELF-SERVICE WEBSITES (BY CODE NUMBERS SHOWN ABOVE) – Where to write/send this form
1
Air Force Personnel Center
HQ AFPC/DPSIRP
550 C Street West, Suite 19
Randolph AFB, TX 78150-4721
6
National Archives & Records Administration
Research Services (RDT1R)
700 Pennsylvania Avenue NW
Washington, DC 20408-0001
11
Department of Veterans Affairs
Records Management Center
ATTN: Release of Information
P.O. Box 5020
St. Louis, MO 63115-5020
2
Air Reserve Personnel Center
Records Management Branch (DPTSC)
18420 E. Silver Creek Avenue
Building 390 MS 68
Buckley AFB, CO 80011
7
US Army Human Resources Command’s web page:
https://www.hrc.army.mil/TAGD/Accessing%20or%20
Requesting%20Your%20Official%20Military%20Pers
onnel%20File%20Documents
or 1-888-ARMYHRC (1-888-276-9472)
12
Division of Commissioned Corps Officer Support
ATTN: Records Officer
1101 Wooton Parkway, Plaza Level, Suite 100
Rockville, MD 20852
3
Commander, Personnel Service Center
(BOPS-C-MR) MS7200
US Coast Guard
2703 Martin Luther King Jr Ave SE
Washington, DC 20593-7200
MR_CustomerServ[email protected]
8
Navy Medicine Records Activity (NMRA)
BUMED Detachment St. Louis
4300 Goodfellow Boulevard, Building 103
St. Louis, MO 63120
13
AF STR Processing Center
ATTN: Release of Information
3370 Nacogdoches Road, Suite 116
San Antonio, TX 78217
14
National Personnel Records Center
(Military Personnel Records)
1 Archives Drive
St. Louis, MO 63138-1002
eVetRecs:
http://www.archives.gov/veterans/military-service-records/
4
Headquarters U.S. Marine Corps
Manpower Management Records & Performance
(MMRP-10)
2008 Elliot Road
Quantico, VA 22134-5030
9
AMEDD Record Processing Center
3370 Nacogdoches Road, Suite 116
San Antonio, TX 78217
5
Marine Forces Reserve
2000 Opelousas Avenue
New Orleans, LA 70146-5400
10
Navy Personnel Command (PERS-313)
5720 Integrity Drive
Millington, TN 38055-3120
